
Compelling Vitamin B12 Research
Wide ranging vitamin B12 research shows the prominent role of vitamin B12 in maintaining health, even before birth, as well as reducing unwanted outcomes from diabetes, depression, even brain atrophy.
B12 and Pregnancy ~
“Before becoming pregnant, women need to get enough vitamin B12 to cut their risk of having a baby with a serious birth defect of the brain and spinal cord… Irish women with the lowest vitamin B12 levels were five times more likely to have a baby with a neural tube defect than those with the highest levels… Neural tube defects can lead to lifelong disability or death.”
The most common birth defects of the brain and spinal cord are spina bifida, in which the spinal cord and back bones do not form properly, and anencephaly, a fatal condition in which the brain and skull bones do not develop normally. Dr. James Mills, U.S. National Institutes of Health. Pediatrics, March 2009.
“An absolutely critical point is that women have to consider this before they become pregnant because once they realize they are pregnant it’s likely to be too late,” Mills said in a telephone interview.
The study involved almost 1,200 women in Ireland who gave blood samples during early pregnancy, which were analyzed to determine vitamin B12 levels. The women in the lowest 25 percent of vitamin B12 levels were five times more likely than those in the highest 25 percent to have had a baby with a neural tube defect.
The researchers suggested that women have vitamin B12 levels above 300 nanograms per liter before getting pregnant. Dr. James Mills, U.S. National Institutes of Health. Pediatrics, March 2009.

.Methyl-B12 1,000 mcg 100 lozenges

Vitamin B12 research re Diabetes
B12 and Leg Symptoms in Diabetes ~
“Symptoms in the legs, such as paresthesia, burning pains, and heaviness, dramatically improved. The effect appeared within a few hours to one week and lasted from several months to four years.” Clinical usefulness of intrathecal injection of methylcobalamin in patients with diabetic neuropathy; Clinical Theraputics, 1987, researchers Ide H, Fujiya S, Asanuma Y, Tsuji M, Sakai H, Agishi Y.
Be aware that Methylcobalamin lozenges work as well as, or better, than injections.
Vitamin B12 Research re Nerve Regeneration in Diabetes ~
“An ultra-high dose of vitamin B12 has been reported to promote peripheral nerve regeneration in experimental neuropathy. METHODS: Nine patients received a 500 microg methylcobalamin injection 3 times a week for 6 months. The effects were evaluated using neuropathic pain grading and a nerve conduction study. RESULTS: Serum concentrations of vitamin B12 were ultra-high during treatment due to the lack of urinary excretion. After 6 months of treatment, the patients’ pain or paresthesia had lessened, and the ulnar motor and median sensory nerve conduction velocities showed significant improvement. There were no side effects.” Intravenous methylcobalamin treatment for uremic and diabetic neuropathy in chronic hemodialysis patients. Internal Medicine, Japan, 1999, research by Kuwabara S, Nakazawa R, Azuma N, Suzuki M, Miyajima K, Fukutake T.
My holistic M.D. prescribed a shot a day, for a year, which I found unbelievable until I began using it and peripheral neuropathy I’d had for years went completely away, but not over-night.
“Seven men and four women with symptomatic diabetic neuropathy were treated with Methylcobalamin (2,500 micrograms in 10 ml of saline) injected intrathecally… Symptoms in the legs, such as paresthesia, burning pains, and heaviness, dramatically improved… ” Methylcobalamin in spinal fluid was 114 +/- 32 pg/ml before intrathecal injection (n=5) and 4,752 +/- 2,504 pg/ml one month after… Methylcobalamin caused no side effects. Clinical usefulness of intrathecal injection of Methylcobalamin in patients with neuropathy – Ide H Fujiya S Asanuma Y Tsuji M Sakai H Agishi Y, Clin Ther (1987)
Diabetic neuropathy in cats ~
Incidentally, I received an email on February 10, 2008, relating to methyl-B12 healing diabetic neuropathy in cats. I had run across a web site about this and written to the webmaster.
Laurie, the site owner, responded, “Goodness, cats can take as much as 25 MG of methylcobalamin with no problem. Through Jasper’s site, I’ve been in touch with thousands of people over the years, and some only needed to give their cats 3 to 6 MG per day, others needed more. An average, I’d say, is 12 MG – and that’s factoring in people whose cats’ diabetes is not regulated, so they’re fighting ongoing damage and need more of the vitamin to help them.”
What is astonishing to me about that “informal research”, and WONDERFUL, is that it is exactly what I found when I got rid of my peripheral neuropathy when I was having a B12 shot a day, which is about the same as 25 to 30mg of methylcobalamin a day in lozenges.
Not “exactly”, because a cat is tiny and I am 6 feet tall and heavy. 2008, Karen Kline

Vitamin B12 research re Depression
B12 and Depression ~
“Depression seems characteristic of most vitamin B deficiencies.” British Journal of Psychiatry. June 1990.
Low B12 and Severe Depression ~
“In community-dwelling older women, metabolically significant vitamin B(sub 12) deficiency is associated with a twofold risk of severe depression.” Vitamin B12 deficiency and depression in physically disabled older women: epidemiologic evidence from the Women’s Health and Aging Study. American Journal of Psychiatry. May 2000. (Authors include Stabler)
B12 and Bereaved Men ~
“An examination of the relationship of plasma cobalamin (vitmin B(12)) level to overall psychological distress, specific mood states, and major depressive disorder was conducted in 159 bereaved men… findings suggest that cobalamin level may be physiologically related to depressed and anxious mood level, as well as to syndromal depression… Cobalamin level is related to self-reported and clinically rated mood and to syndromal…” Health Source – Consumer Edition, 2000.
 Antidepressants and B12 ~
Antidepressants and B12 ~
Practice Guidelines for prescribing antidepressants suggest that antidepressants won’t work as well until the B12 level is higher than 400. Emily Deans, psychiatrist blog, 2010. Read more.
Vitamin B12 research re deficiency and age
Low B12, Age, and Mental Impairment ~
“Cobalamin deficiency worsens with increasing age and has been implicated in declining cognitive functions in elderly persons. Early diagnosis and treatment of cobalamin deficiency are thus important in preventing or slowing down neuropsychiatric disorders in the elderly.” Review: cobalamin deficiency and mental impairment in elderly people, Age and Ageing, Nov. 1995.
“Cobalamin deficiency increases with advancing age and is found in 3% to 42% of persons aged 65 and over.” Ibid.
“It has been shown that nearly 50% of patients with low serum cobalamin and a normal Schilling test are unable to absorb protein-bound cobalamin as opposed to the free cobalamin used in the Schilling test.” Ibid.
“Another manifestation of cobalamin deficiency is altered mental status, which consists of impairment of attention span, memory abstraction, or other intellectual functions with or without abnormalities of behaviour, mood, affect, or logical thought. Neuropsychiatric symptoms may be the initial, or the only, manifestations of cobalamin deficiency.” Ibid.
“Cobalamin deficiency may result in a variety of mental symptoms, such as organic psychosis, dementia paranoia, memory impairment, mania, slow mentation, hallucinations, and depression.” Ibid.
“A finding of low serum cobalamin levels in Alzheimer’s disease and multi-infarct dementia, but not in other forms of dementia or cognitive impairment, would suggest that cobalamin deficiency may cause specific types of dementia and is not the result of dementia with consequently insufficient dietary intake of cobalamin.” Ibid.
“In a recent study 18 subjects with low serum cobalamin and evidence of cognitive dysfunction were investigated. Only patients who had symptoms for less than 1 year showed improvement after therapy. The best clinical responders had been symptomatic for less than 6 months.” Ibid.
“These investigations indicate that the duration of the cobalamin deficiency plays an essential role in the degree of improvement of neuropsychiatric symptoms after treatment.” Ibid.
“This is important, because cobalamin deficiency may have to be acknowledged as a significant cause of neuropsychiatric disorders in elderly people. Early treatment may prevent irreversibility of the neuropsychological features and organic lesions of the brain related to the deficiency.” Ibid.
I find the above not entirely convincing. I had B12 shots and used lozenges for over a decade before I learned that all B12 is made by micro-organisms, the very same ones that are used to culture Swiss cheese. These bacteria make not only the holes in Swiss cheese, but vitamin B12. After learning this I began eating a few ounces of Swiss cheese a day, and had more memory improvement than I’d had in the preceeding 10 years. The reason for the increased improvement, I believe, is that though the bacteria make a tiny amount of B12 as they live in our digestives system, they do it round the clock… from things like tomatoes, all sorts of things that don’t have any B12 in them. The constancy appears to result in B12 getting back into deep tissue.

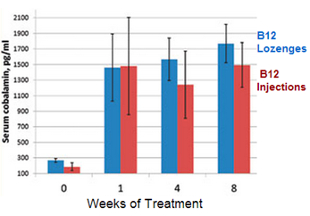
Vitamin B12 research re lozenges vs shots
High Dose B12 Lozenges Are Effective ~
Effectiveness of high-dose methylcobalamin lozenges in treating vitamin B12 deficiency is confirmed in findings presented at the 2012 Conference of the American Association of Naturopathic Physicians.
In this clinical trial, 10 patients with newly diagnosed cobalamin deficiency were randomly assigned to receive either once-a-week B12 injections (1,000 mcg) or daily high-dose 10,000 mcg methylcobalamin lozenge for eight weeks.
The study showed vitamin B12 lozenges were as effective as injections. Both treatments resulted in complete normalization of serum cobalamin levels in all patients. Importantly, homocysteine levels returned to normal and general symptoms improved regardless of type of treatment.
Results showed daily high-dose methylcobalamin lozenges are a viable, convenient alternative to B12 shots and are equally effective. Additionally, lozenges offer a significant cost advantage. Effect of Daily High-Dose Methylcobalamin Lozenge Regimen or Weekly Injections in Patients with Cobalamin Deficiency. A Single-Center Prospective Randomized Open-Label Trial. Culik DA BL, Sharpee RL, Pacholok SM. AANP 2012 Conference. Read more.
Vitamin B12 research re pernicious anemia
B12 and Pernicious Anemia ~
“Pernicious anemia results from a deficiency of cobalamin, or vitamin B12. The neurological symptoms associated with cobalamin deficiency were identified more than 100 years ago. Today, cobalamin deficiency is more likely to be recognized in its earlier stages, and the associated neurological symptoms are more easily reversed by vitamin B12 treatment.” Neurologic aspects of cobalamin deficiency, Medicine, July 1991, research by: Heaton, Savage, Brust, Garrett, Lindenbaum.
Vitamin B12 research re nerves and brain
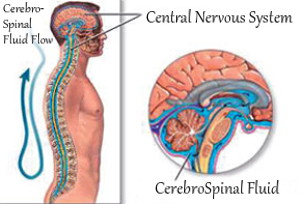
Low B12 and Cerebrospinal Fluid ~
“Among patients with cobalamin deficiency, the blood level of methylmalonic acid was about eight times greater than among controls. However, in the cerebrospinal fluid, the level of methylmalonic acid was, on the average, 600 times greater than among control patients.” Ibid.
Google AI, on methylmalonic acid: Elevated levels of methylmalonic acid (MMA) can have various effects, including vitamin B12 deficiency. In cases of MMA accumulation, it can lead to brain damage, developmental delays, and other serious health complications. Additionally, MMA is a biomarker for mitochondrial dysfunction and has been linked to various diseases and conditions.
Low B12 and Brain Atrophy ~
Over 5 years in a community population of 107 elderly, the lower the B12 status, the faster the brain atrophied. Vogiatzoglou, Refsum, Johnston, et al. Vitamin B12 status and rate of brain volume loss in community-dwelling elderly. Neurology 2008;71:826–32.
Low B12 Affects Cognitive Function in Adolescents ~
“The objective of this study was to investigate whether cognitive functioning is affected in adolescents (aged 10-16 y) with marginal cobalamin status as a result of being fed a macrobiotic diet up to an average age of 6 y… Conclusion: Our data suggest that cobalamin deficiency, in the absence of hematologic signs, may lead to impaired cognitive performance in adolescents.” American Journal of Clinical Nutrition. Sept. 2000.
B12 and Dementia Improvement ~
“Patients with mild-moderate dementia and elevated plasma homocysteine levels improved clinically with increased test scores after vitamin substitution.” Improvement of cognitive functions after cobalamin/folate supplementation in elderly patients with dementia and elevated plasma homocysteine. AlternativeMedicine Review. Oct. 2001.
B12 and Improved Cognitive Function ~
“Mild cobalamin (Cbl) deficiency is frequently found in older persons and is associated with cognitive and cerebral abnormalities… Conclusion. Electrographic signs of improved cerebral function and improved cognitive function were found after Cbl supplementation in older subjects with low plasma Cbl concentrations who were free of significant cognitive impairment. These improvements were related to a reduction of plasma tHcy concentration.” Cobalamin supplementation improves cognitive and cerebral function in older, cobalamin-deficient persons. The Journals of Gerontology, Series A. Dec. 2001.
Low B12 and Predicting Cognitive Dysfunction ~
“Elevated metabolites of the enzyme cofactor cobalamin in elderly patients may predict the future development of cognitive dysfunction, especially in men, according to a study presented at the annual meeting of the American Geriatrics Society. High levels of methylcitric acid and, to a lesser degree, other cobalamin (vitamin [B.sub.12] metabolites correlated significantly with lower scores on many sections of the California Verbal Learning Test (CVLT), reported Dr. Angela Garcia of Queen’s University, Kingston, Ont.” Cobalamin markers could signal cognitive decline. (Nondemented Elderly Patients). Family Practice News. Oct. 2002.
B12 and Abnormalities in Blood and Neurological Function ~
“Vitamin B12 deficiency causes abnormalities in both the blood and in neurological function. In many patients, the neurological abnormalities resulting from vitamin B12 deficiency become apparent before any blood abnormalities develop. These neurological abnormalities may cover a wide spectrum, ranging from abnormal sensations and impairment of vibration, to conditions as severe as abnormal gait and even dementia.” Cerebrospinal fluid methylmalonic acid levels in normal subjects and patients with cobalamin deficiency, by Stabler, Allen, Barrett, Savage, Lindenbaum. Neurology. Oct. 1991.
Neurological Symptoms ~
“Of 369 patients with documented cobalamin deficiency seen over a 17-year period, 189 developed neurological symptoms. In 114 cases, the neurological symptoms were the first indications of the vitamin deficiency. The most common initial complaint was paresthesia, or abnormal sensation, which affected more than 70 percent of the patients with neurological symptoms. These abnormal sensations took the form of a ‘pins and needles’ feeling, numbness, or tingling. In 10 cases, these feelings were strong enough to be considered disabling by the patient. In 122 episodes of deficiency, neurological abnormalities were found at the time of initial diagnosis. The most common was reduced sensitivity to vibration, which was observed in 107 episodes. Proprioception, the awareness of position and movements of the body, was impaired or absent in the toes or ankles in 72 episodes.”
“The majority of cases improved with treatment; moderate or severe neurologic disability was known to persist in only 6.3 percent of the patients who received adequate follow-up. Eleven of the 18 patients with mental impairment had a complete response to vitamin B12 therapy.” Ibid.
“The extent of nervous system dysfunction was clearly related to the duration of neurologic symptoms before treatment.” Ibid.
“In the 10 episodes in which the pretreatment severity score was 20 or greater a complete response was seen in only 2 and residual neurologic dysfunction was observed in all of the 8 episodes in which the severity score was more than 23 before therapy.” Ibid.
“Duration of symptoms correlated quantitatively with post-treatment severity.” Ibid.
“When mental impairment occurred, however, it was frequently the most disabling and dominant neurologic abnormality.” Ibid.
![]() “A striking feature of our patients was the high degree of responsiveness to Cbl [cobalamin] therapy.” Ibid.
“A striking feature of our patients was the high degree of responsiveness to Cbl [cobalamin] therapy.” Ibid.
“The severity score was reduced by 50% or greater after treatment in 91% of the episodes. Residual long-term moderate or severe neurologic disability was noted following only 7 (6.3%) episodes.” Ibid.

Recurrent seizures: an unusual manifestation of vitamin B12 deficiency
The present report highlights an unusual presentation of vitamin B12 deficiency–recurrent seizures in a 26-year-old man. His symptoms responded to parenteral vitamin B12 therapy. Neurol Ind. 2004, Mar.
2008 ~ Speaking for myself ~
From countless observations it appears that vitamin B12 and fingernails are linked. In fact, it appears that our fingernails reveal low vitamin B12 health issues. That doesn’t mean, however, that ridges on fingernails of the loss of moons are the only low B12 symptoms to consider. If you have a low B12 health problem then you will most certainly have other symptoms as well as those visible in your fingernails, and I’m guessing that you’ve already checked a list of symptoms of low vitamin B12. To understand the relationship between your symptoms and a low B12 level, it’s good to read vitamin B12 research, or at least excerpts from it, like those on this page.
Vitamin B12 research re causes of deficiency
Causes of low vitamin B12 levels ~
“Classical disorders such as pernicious anemia are the cause of this deficiency in only a small proportion of the elderly. A more frequent problem is food-cobalamin malabsorption which usually arises from atrophic gastritis and hypochlorhydria but other mechanisms seem to be involved in some patients.” Cobalamin,the stomach, and ageing. American Journal of Clinial Nutrition. Oct. 1997.
“The partial nature of this form of malabsorption produces a more slowly progressive depletion of cobalamin than does the more complete malabsorption engendered by disruption of intrinsic factor-mediated absorption. The slower progression of depletion probably explains why mild, preclinical deficiency is associatedwith food-cobalamin malabsorption more often than with pernicious anemia.” Ibid.
Low B12 and h.pylori ~
“Evidence for vitamin [B.sub. 12] deficiency usually involves combinations of low serum vitamin [B.sub.12] levels, clinical and metabolic abnormalities, and therapeutic response. Identification of the underlying cause is important in the diagnosis of vitamin[B.sub. 12] deficiency that is usually attributed to malabsorption. Helicobacter pylori is one of the most common causes of peptic ulcer disease worldwide and a major cause of chronic superficial gastritis leading to atrophy of gastric glands. It is suggested that there may be a causal relationship between H pylori and food cobalamin malabsorption.” Helicobacter pylori–Is It a Novel Causative Agent in Vitamin [B.sub.12] Deficiency? Archives of Internal Medicine. May 2000.
Diarrhea can be a sign of h.pylori interfering with B12 absorption.
“Food cobalamin is released as a stable complex with gastric R binder and its absorption depends on the initial release from the binders in food. Food-cobalamin malabsorption is marked by the inability to release cobalamin from food. Therefore, cobalamin cannot be taken up by intrinsic factor for absorption. Release of cobalamin from food requires acid and pepsin, and most food-cobalamin malabsorptive states can be traced to gastric defects. However, other mechanisms may also play a role.” Ibid.
“It has been proposed that pernicious anemia may represent the final phase of a process that begins with H pylori–associated gastritis and evolves through progressive levels of atrophy until parietal cell mass is entirely lost.” Ibid.
Low B12 Caused by Inability to Release B12 from Food ~
“In a retrospective study that was conducted in 1994 and 1995, we demonstrated that a majority (55%) of cases of cyanocobalamin (vitamin [B.sub.12]) deficiency were related to the inability to release cobalamin from food and that pernicious anemia was a rare condition (17%). In a second retrospective study that was conducted between 1995 and 1998, we confirmed that food cobalamin malabsorption was emerging as a major cause of vitamin [B.sub.12] deficiency. We found that 68 patients (60%) had a vitamin [B.sub.12] deficiency caused by food cobalamin malabsorption and 7 subjects (6%) had pernicious anemia.” Food Cobalamin Malabsorption: A Usual Cause of Vitamin [B.sub.12] Deficiency. Archives of Internal Medicine. July 2000.
“There is little reason to treat food cobalamin malabsorption differently than pernicious anemia.” Ibid.
Challenge of Mild Cobalamin Deficiency ~
“Attention has shifted recently to the challenge of milder cobalamin deficiency states in which signs such as megaloblastic anemia are not apparent. This is a much more common problem than classical deficiency. This entity has emerged largely because of the application of sensitive metabolic tests to patients.” Mild cobalamin deficiency. The Western Journal of Medicine. June 1998.
Megalin and Transcobalamin ~
“Megalin has previously been shown to bind and mediate endocytosis of transcobalamin (TC)-[B.sub.12]. However, the physiological significance of this has not been established, and other TC-[B.sub.12] binding proteins have been suggested to mediate renal uptake of this vitamin complex. The present study demonstrates by the use of megalin-deficient mice that megalin is, in fact, essential for the normal renal reabsorption of TC-vitamin [B.sub.12] and for renal accumulation of this highly conserved vitamin.” Megalin is essential for renal proximal tubule reabsoption and accumulation of transcobalamin-[B.sub.12]. The American Journal of Physiology. March 2002.
Prescriptions causing low vitamin B12 levels
Vitamin B12 deficiency, even the advanced stage of megaloblastic anemia, may occur with the use of anticonvulsants and/or oral contraceptives. Drugs, toxins and dietary amino acids affecting vitamin B12 or folic acid absorption or utilization, American Journal of Medicine, 1970.
Proton pump inhibitors (PPI) are one of the most widely used classes of drugs. PPIs have a favorable safety profile. However, with increasing numbers of patients chronically taking PPIs for gastroesophageal reflux disease and other common, persistent conditions, the long-term potential adverse effects are receiving increasing attention. An area receiving much attention is the long-term effect of chronic acid suppression on the absorption of vitamin B12 and the minerals magnesium and calcium. Association of Long-Term Proton Pump Inhibitor Therapy with Bone Fractures and Effects on Absorption of Calcium, Vitamin B12, Iron, and Magnesium, Current Gastroenterology Reports, 2010.
Megaloblastic anaemia from taking anticonvulsant drugs phenytoin or primidone. Vitamin B12 absorption in the megaloblastic anaemia caused by anticonvulsant drugs. Quarterly Journal of Medicine.
Vitamin B12 research re ALS
Methylcobalamin slows ALS ~
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disorder affecting both upper and lower motor neurons… We have shown the ultra-high-dose methylcobalamin (25 mg/day i.m.) slows down the progressive reduction of the CMAP (compound muscle action potential) amplitudes in ALS in the short term (4 weeks). The latencies of SSR (sympathetic skin response) were shorter after treatment (50 mg/day i.v., 2 weeks). In the long-term effect of methylcobalamin (50 mg/day i.m., twice a week), the survival time (or the period to become respirator-bound) was significantly longer in the treated group than in the untreated. Clinical trials of ultra-high-dose methylcobalamin in ALS – Izumi Y, Kaji R. Brain Nerve (2007)
Research linking low B12, high homocysteine, and heart disease
Healthy B12 levels ~
Research has found that mental impairment begins at vitamin B12 levels of 500-550. The U.S. low is 350 points below that, so Americans suffer more health loss before a blood test will alert their doctors to the problem. Read more.